🏥 Boari Flap – Ureteral Reconstruction Technique
The Boari flap is a surgical technique used to reconstruct or replace the distal ureter when a segment is damaged, obstructed, or removed due to trauma, strictures, tumors, or iatrogenic injury.
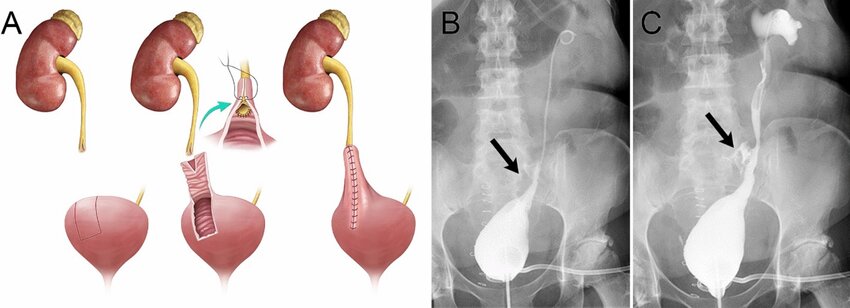
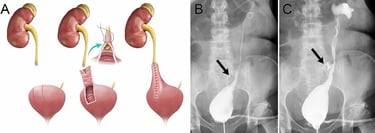
It involves creating a tubular flap from the bladder wall, which is then anastomosed to the remaining healthy upper ureter to bridge the gap and restore urinary continuity.
🧾 Indications
The Boari flap is used when:
There is mid to lower ureteral injury or stricture.
Tension-free ureteral reimplantation is not possible due to ureter length loss.
Long segment ureteral defects (up to 10–15 cm) need bridging.
Following resection of ureteric tumors or damaged segments.
🩺 Surgical Steps (Simplified)
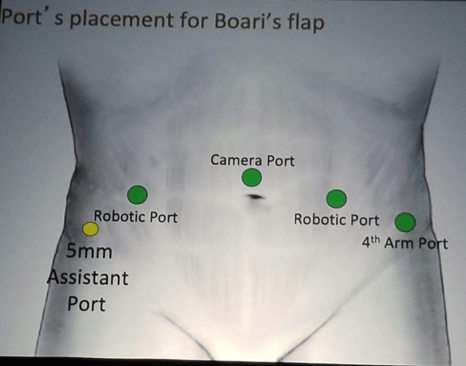
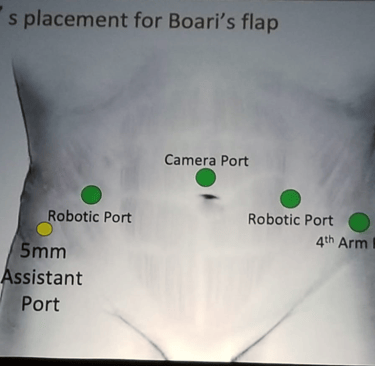
Exposure: Via open, laparoscopic, or robotic-assisted approach.
Mobilization:
The bladder is mobilized and a vascularized flap is created from its anterior or posterior wall.
A psoas hitch may be done if needed to elevate the bladder.
Flap Creation:
A rectangular bladder flap (usually 2–3 cm wide) is constructed and tubularized into a neoureter.
Anastomosis:
The Boari flap is anastomosed end-to-end to the proximal ureter.
Stenting:
A double-J ureteral stent is placed to ensure patency during healing.
Closure:
Bladder is closed; abdominal cavity is closed in layers.
🧪 Postoperative Care
Foley catheter for 7–10 days.
JJ stent removal after 4–6 weeks.
Imaging (e.g., renal ultrasound, CT urogram) to confirm healing and drainage.
Antibiotic prophylaxis if indicated.
Boari flap is a useful option when the diseased segment of the ureter is too long, or ureteral mobility is too limited to perform a primary ureteroureterostomy. Boari flaps can be created to bridge a 10- to 15-cm ureteral defect. If needed, spiral bladder flaps can be constructed to reach the renal pelvis in some circumstances.
The robot is ideal for creating the Boari flap according to Dr. Hemal. It can be used to create the Boari flap up to the level of L3-L4. A cystogram needs to be performed to outline bladder contour and determine its capacity.
The actual technique entails
1. Identification of the ureter at the bifurcation of the common iliac artery or above and mobilization of it caudally until you can identify the stricture site.
2. Mobilization of the bladder as distally as possible on both sides
3. The ratio between the length and width of the bladder flap is 2:1 (classic teaching in open surgery was 5:1).
4. Performing a Psoas hitch is required in every case. A psoas hitch entails mobilization of the bladder with fixation above the iliac vessels to guarantee a tension-free ureteric anastomosis.
5. The ureter is spatulated, and a sub-mucosal tunnel is created at the cranial aspect of the Boari’s flap and the ureter is carefully tunneled through the sub-mucosal tunnel into the bladder.
6. The ureter is then sutured to the mucosa of the flap using interrupted sutures.
7. Tubularization of the bladder flap takes place with continuous sutures placed in two layers.
8. The bladder opening is then closed in two layers using continuous sutures.
9. The watertight suturing of the anastomosis and bladder is finally tested.
Patient Feedback
Read what our satisfied patients say about Dr. Yasir Iqbal Lone.
Dr. Lone provided exceptional care during my surgery. Highly recommend his services!
John Smith
New Delhi
I am thoroughly impressed with Dr. Lone's expertise and caring nature. His staff is friendly, and I felt well taken care of throughout my treatment journey.
Emily Clark
Delhi NCR